
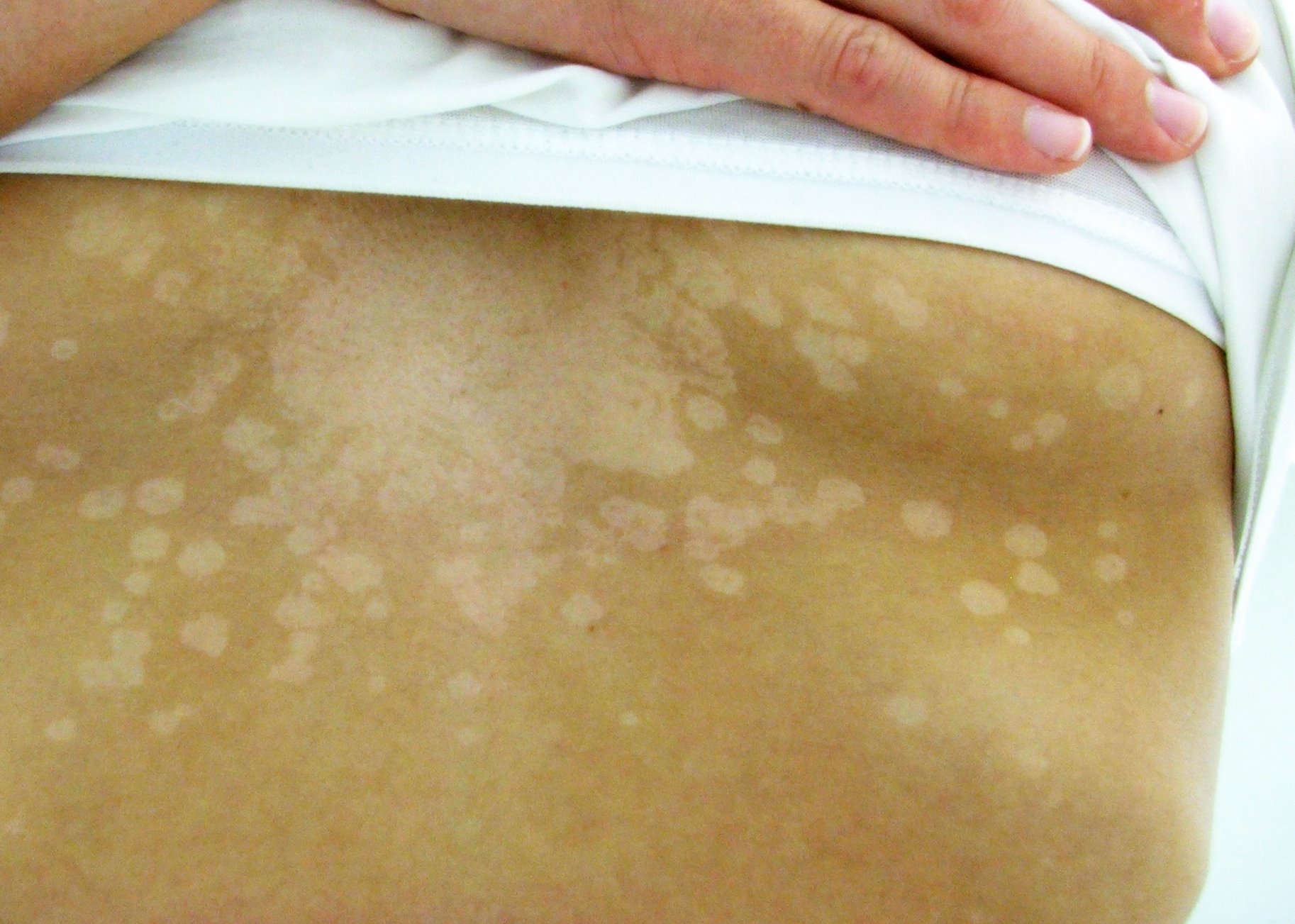
Image: "Tinea versicolor" by Klaus D. Peter, M.D. is licensed under CC BY-SA 3.0. Link to the source.
Tinea Versicolor
Introduction | Aetiology | Clinical Presentation | Diagnosis | Management | Prevention | When to Refer | References
Introduction
Tinea versicolor, also known as Pityriasis versicolor, is a common superficial fungal infection of the skin caused by the yeast Malassezia. It is characterised by patches of discoloured skin, often on the trunk and upper arms. The condition is typically benign and not contagious, but it can cause cosmetic concerns due to the noticeable changes in skin pigmentation.
Aetiology
Tinea versicolor is caused by an overgrowth of Malassezia, a genus of yeast that is part of the normal skin flora. Factors that can promote the overgrowth of this yeast include:
- Hot and Humid Climates: Warm and moist environments encourage the proliferation of Malassezia.
- Oily Skin: Excessive sebum production can create a favourable environment for yeast growth.
- Immunosuppression: Individuals with weakened immune systems, such as those on immunosuppressive therapy or with HIV, are more prone to developing tinea versicolor.
- Hormonal Changes: Adolescents and young adults are more commonly affected, possibly due to hormonal changes that increase sebum production.
- Genetic Predisposition: A family history of tinea versicolor may increase the risk of developing the condition.
Clinical Presentation
Tinea versicolor typically presents with the following features:
- Discoloured Patches: The most characteristic feature is patches of skin that are lighter (hypopigmented) or darker (hyperpigmented) than the surrounding skin. These patches are usually found on the chest, back, upper arms, and neck.
- Fine Scaling: The affected areas may have a fine, flaky scale that is more noticeable when the skin is stretched or scratched.
- Mild Itching: While most cases are asymptomatic, some individuals may experience mild itching, particularly in hot and humid weather.
- Non-Contagious: Tinea versicolor is not contagious and cannot be spread from person to person.
Diagnosis
The diagnosis of tinea versicolor is primarily clinical, based on the appearance of the skin. However, additional tests may be used to confirm the diagnosis:
- Wood's Lamp Examination: Under a Wood's lamp (UV light), the affected areas may fluoresce a yellow-green colour, helping to distinguish tinea versicolor from other skin conditions.
- KOH Preparation: A skin scraping can be examined under a microscope after being treated with potassium hydroxide (KOH). This test reveals the characteristic "spaghetti and meatballs" appearance of the yeast and hyphae.
- Skin Biopsy: In rare cases where the diagnosis is uncertain, a skin biopsy may be performed, though this is usually not necessary.
Management
Tinea versicolor can be effectively treated with topical or systemic antifungal medications:
Topical Treatments
- Antifungal Shampoos: Selenium sulfide 2.5% shampoo, ketoconazole 2% shampoo, or zinc pyrithione shampoo can be applied to the affected areas and left on for 5-10 minutes before rinsing. This is typically done daily for one to two weeks.
- Topical Antifungal Creams: Imidazole creams such as clotrimazole or miconazole can be applied to the affected areas twice daily for two weeks.
Systemic Treatments
- Oral Antifungals: In extensive or recurrent cases, oral antifungals such as fluconazole or itraconazole may be prescribed. Fluconazole 150 mg as a single dose or itraconazole 200 mg daily for 7 days are common regimens.
Post-Treatment Considerations
- Residual Pigmentation: Even after successful treatment, it may take several weeks or months for the skin's normal pigmentation to return. This is because the yeast itself is eradicated, but the skin's pigment production takes time to normalise.
- Recurrence: Tinea versicolor can recur, especially in individuals living in humid climates or those with other risk factors. Maintenance therapy with antifungal shampoos used once or twice a month can help prevent recurrence.
Prevention
To reduce the risk of developing or recurring tinea versicolor, the following preventive measures may be helpful:
- Good Hygiene Practices: Regular washing with antifungal soaps or shampoos, particularly in warm and humid conditions, can help prevent the overgrowth of Malassezia.
- Lightweight Clothing: Wearing loose-fitting, breathable clothing can reduce sweating and limit the warm, moist environment that promotes yeast growth.
- Prophylactic Antifungal Use: In individuals with a history of recurrent tinea versicolor, using antifungal shampoos or creams on a regular basis, particularly during warm months, may help prevent recurrence.
When to Refer
Referral to a dermatologist may be necessary in the following situations:
- Uncertain Diagnosis: If the clinical presentation is atypical or does not respond to initial treatment, further evaluation by a specialist is recommended.
- Recurrent or Extensive Disease: In cases of recurrent tinea versicolor or extensive involvement that does not respond to standard treatments, specialist advice may be required.
- Complications: If secondary infections or other complications arise, referral to a dermatologist is advisable.
References
- British Association of Dermatologists (2024) Guidelines on the Management of Tinea Versicolor. Available at: https://www.bad.org.uk (Accessed: 26 August 2024).
- National Institute for Health and Care Excellence (2024) Management of Superficial Fungal Infections. Available at: https://www.nice.org.uk/guidance/ng59 (Accessed: 26 August 2024).
- British National Formulary (2024) Topical and Oral Antifungal Treatments. Available at: https://bnf.nice.org.uk/ (Accessed: 26 August 2024).




Blueprint Page
Explore the comprehensive blueprint for Physician Associates, covering all essential topics and resources.
Book Your Session
Enhance your skills with personalised tutoring sessions tailored for Physician Associates.